Prior authorization has long been one of the most friction-filled processes in healthcare administration – a burden felt acutely by providers, payers, and ultimately patients. Despite years of industry progress on electronic transactions and data standards, prior authorization workflows remain largely manual, point-to-point, and difficult to administer.
That’s why UHIN is proud to be named a participant in the Da Vinci Trebuchet Clearinghouse-to-Clearinghouse (CH-to-CH) Prior Authorization Pilot, launched by the Cooperative Exchange in collaboration with the HL7® Da Vinci Project. A clearinghouse is a secure network hub connecting thousands of payers and providers to streamline the verification, processing, and exchange of healthcare transactions – including prior authorization.
The pilot brings together eleven clearinghouses – including Waystar, Optum, Availity, Veradigm, and others – to test whether HL7® FHIR®-based prior authorization transactions can be operationalized across clearinghouse networks, not just within individual point-to-point connections. The cohort will also validate hybrid X12 and FHIR translation workflows that reflect how the industry actually operates today. The goal is a functional prototype, a clearinghouse implementation playbook, and concrete recommendations for improving the underlying standards, including Da Vinci, FAST Implementation Guides, and X12.
For UHIN, this work is a natural extension of our mission as the state-designated, nonprofit HIE, the Clinical Health Information Exchange (CHIE), and the nation’s only nonprofit clearinghouse network. For providers UHIN, allows for fewer rejections and reduced friction in the claim lifecycle. For payers, UHIN offers a single connection point for clean data. This enhances the delivery of more complete claims, valid codes, and accurate eligibility information, which reduces costly manual interventions.
Clearinghouses have quietly enabled electronic data exchange that we’ve been using for years. We believe they’ve been underutilized as the interoperability infrastructure they already are, and that solving prior authorization at scale starts with the networks clearinghouses have spent years building. Participating in this pilot puts us at the table where those standards are being shaped, not just adopted.
Reducing administrative burden isn’t just an efficiency goal; it has real consequences for patient care. Delays in prior authorization can mean delayed treatment, and the complexity of the current process consumes resources that could otherwise be directed toward improving outcomes. By helping to develop the technological capabilities needed to improve prior authorizations like CH-to-CH routing, identity resolution, and endpoint discovery, UHIN is helping to make the entire ecosystem work better for everyone. We’ll share what we learn along the way.
Healthcare works best when information moves as seamlessly as care itself.
With the right data and context, decisions are made faster and with greater confidence. When organizations share information responsibly, operations become more efficient. When communities invest in shared infrastructure, everyone benefits.
That’s the promise of healthcare interoperability. Realizing this promise of a fully connected network requires more than just agreeing with the philosophy – it requires organizations to take specific, concrete actions to participate.
A Shared Vision for Better Care
Utah’s healthcare community has long understood something essential: no single organization delivers care alone.
Patients move across settings. Doctors collaborate across systems. Health plans support care across populations. Government partners steward statewide health priorities. Outcomes depend on timely, accurate information wherever care happens or when decisions about patient care are made.
Interoperability makes this possible not by replacing existing systems, but by connecting them. It creates a foundation where information flows securely, consistently, while supporting a myriad of use cases.
This foundation is what UHIN provides today.
Infrastructure That Grows Stronger Together
UHIN operates Utah’s health information highway, the Clinical Health Information Exchange, or, the CHIE.
Utah’s shared infrastructure gives healthcare organizations secure access to comprehensive patient records across organizational boundaries.
Utah’s health information highway is designed to support all organizations who assist in the care, treatment, and health of Utah’s patients, including different providers across different systems to work as a single team to support the care journey of their shared patients. Effective information exchange requires infrastructure that adapts to how different stakeholders actually work: providers making real-time clinical decisions, health plans coordinating care across populations, and public health agencies tracking community-level outcomes.
The CHIE is a Shared Network
Managing dozens of point-to-point integrations is expensive, creates operational drag, and limits visibility across the care continuum. A shared network offers a different model: one connection that enables information to move across care settings, organizations, and systems.
Utilizing the CHIE, clinicians gain access to timely patient context, health plans can better support coordinated care and quality efforts, and public partners gain clearer insight into healthcare activity across the state. This all makes coordination easier to manage at every handoff – Health Plan to Provider, Health Plan to Health Plan, and Health Plans and Providers to Public Health.
Common Governance Instead of Fragmented Agreements
Trust is foundational to healthcare information exchange. The CHIE establishes a consistent, locally governed framework that supports responsible data sharing. Rather than navigating a patchwork of agreements, policies, and exceptions, UHIN welcomes organizations to participate within clear standards that promote accountability, transparency, and confidence across the ecosystem.
You save costs that are related to manually responding to data access and data sharing requests, and eliminate the time and expense spent on multiple legal and data transfer agreements – the CHIE already has them.
Common Stewardship Instead of Vendor Dependency
Infrastructure should serve the community it supports, not shift direction with market cycles or commercial priorities. UHIN operates as a neutral, non-profit utility, ensuring that Utah’s healthcare connectivity remains guided by community needs. Providers, payers, and public stakeholders collectively shape how the network evolves, supporting long-term sustainability and adaptability.
Together, these principles transform interoperability from a technical capability into a shared asset that grows stronger as participation increases.
Help Shape the Future
How do you know if your organization is helping build the healthcare network we all want to improve health outcomes and reduce costs?
To start, you should ask yourself and members of your organization these five questions:
1. Are you realizing the full value of interoperability?
Compare the membership fee to what you would have to pay to establish separate legal agreements and interfaces with each agency that UHIN connects with or manually respond to and submit records requests.
2. Are you using shared data to improve patient outcomes?
Connecting the pipe is the first step to make a real clinical difference. The next step is integrating CHIE data into workflows ensures providers actively use shared context to make smarter, safer decisions.
For example, Granger Medical Clinic used CHIE ADT alerts to grow patient identification from one per week to 750 per month, cutting readmission rates by 61%.
Tanner Clinic and Connect TCM brought their average readmission rate down to 4% — far below Utah’s 13.9% and the national average of 14.6%.
3. Are you actively sharing?
Passive consumption helps one organization; active sharing strengthens care coordination, improves outcomes, and elevates the entire system. Sending ADT feeds, lab results, and patient records in real time ensures everyone has the information they need, when they need it. Sharing a comprehensive, high-quality record empowers better clinical decisions and reduces gaps in care.
4. How is this community asset funded?
Your financial support through donation or membership sustains the maintenance, innovation, and long-term growth of the data sharing infrastructure that serves us all. UHIN also applies for grants to support the important work the CHIE provides to our community.
5. Do you want to be more engaged, but don’t know how?
For Current CHIE Users: Assess if your organization is helping shape the future of interoperability by asking yourself the questions above. Then, log in at www.uhin.org today to experience the modernized CHIE Platform firsthand. If you need a hand with your account, please contact customer support.
For Former CHIE users or New Organizations: Visit the CHIE Platform page to get the information you need to get started. If you’re ready to connect to the CHIE, you can get started here.
The value to the community of the exchange is realized when every participant holds themselves accountable to these standards. Organizations that ensure their data is timely, complete, and accurate (and who financially support the infrastructure) are the ones shaping the future of Utah healthcare interoperability.
To join this vital cause, organizations must implement the following concrete steps:
1. Move from consumption to contribution: Care does not begin or end within organizational boundaries. The network is strongest when you contribute the timely, complete, and accurate data that the next provider in the chain needs. Organizations must connect to the CHIE and actively share data, specifically by setting up ADT feeds, patient records, and lab results.
2. Align your care teams: Healthcare is a team effort. Shared infrastructure enables collaboration, but only if your internal workflows support it. Ensure your teams are utilizing the data available in the CHIE to gain a complete picture of patient history.
3. Tackle community challenges together: Leaders who build community infrastructure recognize that progress accelerates when stakeholders work from a shared foundation. Participation strengthens not only individual organizations but the resilience and responsiveness of Utah’s healthcare system as a whole.
4. Commit to the infrastructure: If you are relying on the network but not supporting it, becoming a paying member ensures this resource remains available and robust for the long term.
These leadership choices shape how care is delivered today and how it will evolve tomorrow.
A New Chapter for the CHIE
For organizations that have connected to the CHIE in the past, now is the time to take a fresh look.
UHIN’s platform has been modernized and enhanced to better support today’s care delivery needs. The CHIE is more capable, FHIR-aligned, and better positioned to scale as the healthcare community grows. The CHIE is working to assess statewide membership and data quality to improve the data available to the community. Providers, health plans, and public partners engaging with the CHIE today are experiencing a network designed for the future of healthcare in Utah.
If you’ve tried it before, you may be surprised by how much better it is now.
Across Utah, organizations are already using shared infrastructure to support care delivery, coordination, and statewide initiatives.
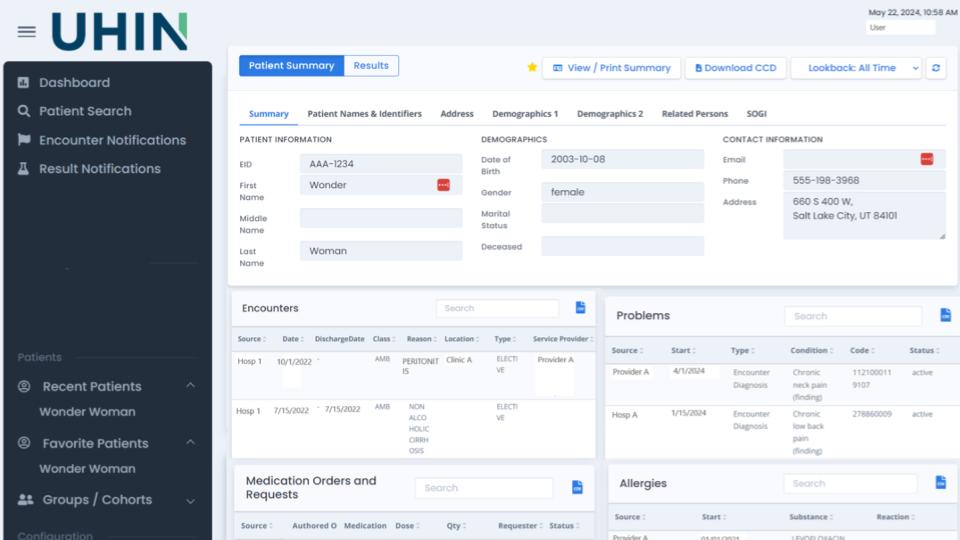
New CHIE Dashboard
Moving Forward, Together
Behind every data feed, every alert, and every shared record is a patient whose care depends on a connected, informed care team. Utah’s information highway is in place. Its power is unlocked when every organization on the care continuum commits to using it fully. That’s how interoperability becomes more than a technical achievement — it becomes a promise kept to the people we serve.
Here is how to get involved:
For Current CHIE Users: Assess if your organization is helping shape the future of interoperability by asking yourself the questions above. Then, log in at www.uhin.org today to experience the modernized CHIE Platform firsthand. If you need a hand with your account, please contact customer support.
For Former CHIE users or New Organizations: Visit the CHIE Platform page to get the information you need to get started. If you’re ready to connect to the CHIE, you can get started here.
UHIN Supports Statewide Effort to Improve Chronic Kidney Disease Detection and Care in Utah.
The Utah Health Information Network (UHIN) is collaborating with Comagine Health, the Utah Department of Health and Human Services (DHHS), and the One Utah Health Collaborative to relaunch the Utah Chronic Kidney Disease (CKD) Coalition. The coalition is focused on improving early detection and management of CKD across the state, using data to inform and support its strategies.
UHIN’s Utah Clinical Health Information Exchange (CHIE) is being used to help develop an alert system that will notify primary care providers when lab results suggest CKD but no diagnosis has been recorded. This alert system is designed to help improve follow-up and diagnosis rates—addressing the reality that 50% of individuals screened for CKD currently do not receive a formal diagnosis or follow-up care.
Additionally, UHIN is evaluating aggregate health data to support early intervention strategies based on methodologies from the National Kidney Foundation. The coalition is exploring the potential for DHHS grant funding to support the implementation of these strategies if data and provider interest support it.
The broader initiative also includes supporting local health districts and clinics in their CKD care efforts and expanding awareness and education around treatment options for end-stage renal disease, such as home hemodialysis and peritoneal dialysis.
UHIN’s involvement is centered on providing the data and tools needed to help health care partners make earlier, more informed decisions in CKD care.
UHIN has played a pivotal role in a recent Centers for Disease Control and Prevention (CDC) project aiming to track the burden, distribution, and impact of Post-COVID conditions (PCC) in Utah. This initiative, detailed in a study published in BMC Public Health, leverages electronic health records (EHRs) and data from The CHIE (Clinical Health Information Exchange) to identify and analyze cases of PCC, commonly known as long COVID. Researchers aim to understand the prevalence, demographic distribution, and healthcare utilization patterns associated with PCC.
The study provides insights into the long-term effects of COVID-19 and highlights the importance of continuous surveillance to address the ongoing health challenges posed by the pandemic.
UHIN, as the only HIE in Utah, was an important contributor to this research. Since 1993, we have been committed to reducing healthcare costs and improving the quality of care through secure electronic data interchange. Our extensive network connects healthcare insurers, physicians, hospitals, laboratories, local health departments, and state agencies, enabling seamless data sharing across the state’s healthcare ecosystem.
In this project, UHIN provided a limited dataset including PCC cases and patient trajectories over time. By providing a limited dataset, UHIN was able to support the project, as allowed under HIPAA, while maintaining patient privacy and data integrity.
Collaborative Approach
A collaborative approach fostered partnerships among various healthcare entities, facilitating the aggregation of diverse data sets. Partners in this work are BeyondHIE, Indiana University, Boise State University, the Bronx Regional Health Information Organization (Bronx RHIO) and Comagine Health (our affiliate partner). This inclusivity enabled a more comprehensive understanding of PCC, as data from different sources provided a holistic view of patient experiences and outcomes. UHIN’s commitment to interoperability and data standardization was key to harmonizing information from multiple providers, ensuring consistency and reliability in the study’s findings.
In Conclusion
The success of this project underscores UHIN’s vital role in national health initiatives. By serving as a central hub for health information exchange, UHIN not only supports clinical care but also empowers research efforts that address pressing health concerns. Our infrastructure and expertise in data management are assets in the ongoing battle against COVID-19 and its long-term effects.
Our involvement in this PCC surveillance project adheres to our mission to enhance healthcare through innovation, collaboration, and inclusiveness. By providing the tools and frameworks necessary for comprehensive data analysis, we are proud to continue to contribute significantly to public health research and the improvement of patient care.
We’re thrilled to share highlights from last year and our early successes in this new year as we work to shape the future of healthcare IT. Keep reading for our 2024 year end recap, Ryan McLelland’s recent participation in Civitas’ FHIR webinar, driving progress with the One Utah Health Collaborative, and making a positive impact for our customers, partners, and community in 2025.
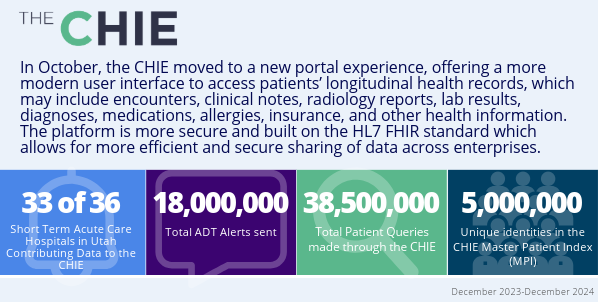
Unwrap an exciting year all in one infographic. We announced our affiliation with Comagine Health and launched the new CHIE portal. We re-invested 100% of our net income to enhance our products and services and achieved a remarkable 95% customer satisfaction rate.
Our Clearinghouse solution processed 329 million transactions, while the CHIE supported 33 of 36 short-term acute care hospitals in Utah, and delivered over 18 million ADT alerts. Click below and unwrap even more from 2024.
Did you miss any of our blog posts from last year? Head to the UHIN blog for valuable insights and perspectives on a variety of topics, like FHIR, cybersecurity, the power of resilient healthcare technology systems, Health Data Utilities, the ideal clearinghouse for providers, virtual payer panel recaps, and more!
We’re proud to be a member of the One Utah Health Collaborative’s Stakeholder Community Board, which includes other notable stakeholders from across the state. Together, we’re driving alignment and progress toward advancing the Utah Model of Care and the 2025 strategic priorities to commit, plan, and act.
We will attended the X12 Winter Standing Meeting in Philadelphia, PA from February 2-6.
We will sponsor the Aspen Grove Provider Fair in Orem, UT on February 7.
Our offices will be closed on February 17 for President’s Day.
Trainings and Webinars
Ryan McLelland on the FHIR Deep Dive Webinar
CIVITAS invited our CTO, Ryan McLelland, to participate in their “FHIR Deep Dive Series” earlier this month. He shared our exciting progress on a state-wide pilot program to create cohesive FHIR-based ecosystems in Utah supported by Da Vinci Trebuchet and eHealth Exchange. Click below to watch!
Comagine Health & CMS Partnership to Strengthen Healthcare for AIAN Communities
Congratulations to our affiliate partner, Comagine Health, for their continued partnership with the Centers for Medicare & Medicaid Services (CMS) in advancing the American Indian/Alaska Native (AIAN) Quality Improvement (QI) Program. The newly awarded contract builds upon previous CMS-funded work with Indian Health Service (IHS) hospitals and providers in 261 facilities within IHS, tribally managed health care facilities, Urban Indian Organizations (UIOs) and CMS-designated nursing homes across the nation.
2024 was a year of reinvestment, growth, and impactful partnerships for UHIN. We dedicated 100% of our net income to enhancing the products and services on which our clients rely, achieving a remarkable 95% customer satisfaction rate. Our Clearinghouse solution processed 329 million transactions, while the CHIE supported 33 of 36 short-term acute care hospitals in Utah, and delivered over 18 million ADT alerts. Key milestones included our affiliation with Comagine Health to drive actionable health insights and the launch of a modernized CHIE portal built on the HL7 FHIR standard for improved data sharing (Learn more about the CHIE portal experience here).
As we reflect on 2024’s successes, we are energized to take on 2025, poised for even greater growth and impact in healthcare.
As the end of the year approaches, we’d like to thank you for being a valued partner in advancing healthcare connectivity. Please keep scrolling for dates that our Customer Support will be closed during the holidays.
In this newsletter: Explore the transformative potential of Health Data Utilities (HDUs), contribute to the draft HDU Framework Supplement, watch the final Virtual Payer Panel of the year, catch up on Ryan McLelland at the eHealth Exchange Annual Meeting, and share your ideas for this newsletter. We wish you a happy and healthy season ahead!
With the holiday season surrounding us with warmth and reflection, we want to take a moment to express our heartfelt gratitude. At UHIN, we deeply care about our customers, our community, and our colleagues. We’re honored to partner with you in advancing healthcare connectivity. From all of us at UHIN, we wish you a season filled with joy, peace, and togetherness.
UHIN’s Customer Support will be closed on the following days:
Tuesday, December 24th
Wednesday, December 25th
Wednesday, January 1st
From the UHIN Blog
What is a Health Data Utility
Health Data Utilities (HDUs) are the next phase for Health Information Exchanges (HIEs), with the goal of utilizing data for purposes beyond basic patient lookup, such as quality improvement, population health, and research. In this post, Navina Forsythe (Chief Data & Privacy Officer) details how HDUs can combine clinical data with other sources like claims and social determinants of health to create comprehensive datasets and foster whole-person care. She also explains the necessary conditions for establishing a HDU, including shared vision, political will, stakeholder participation, legal frameworks, data privacy and security, and funding.
Call for Public Comment: HDU Framework Supplement Version 1
Civitas Networks for Health invites public comment on the draft HDU Framework Supplement Version 1, which outlines critical updates to the existing Health Data Utility Framework. This supplement highlights actionable strategies for advancing health data governance, interoperability, and equity across states and regions. The comment deadline is January 31, 2025.
Ryan McLelland, UHIN’s CIO, participated on the “The “007” of the CMS-0057 Prior Authorization Rule Requiring FHIR” panel at the eHealth Exchange Annual Meeting in Nashville on December 10th.
Trainings and Webinars
Final Virtual Payer Panel of 2024
We hosted our final payer panel of the year with Korey Marsh and Lisa Varley of DMBA who shared important information about new medical plans rolling out on January 1st and answered questions about prior authorization, coding, and more. Thank you to Korey, Lisa, and everyone who participated!
Top Questions and Answers from the Virtual Payer Panel with Korey Marsh and Lisa Varley (both of DMBA)
In our final virtual payer panel in 2024, DMBA representatives Korey Marsh, Manager of Network Strategy and Provider Relations, and Lisa Varley, Director of Configuration, shared key updates for providers. Highlights included an overview of DMBA’s provider portal, which offers tools for pre-authorizations, claims searches, and remittance tracking, with plans for expanded functionality. DMBA also announced the rollout of four new medical plans, including PPO and HSA options, set to replace their existing plans in 2025. Additionally, DMBA addressed questions on coding and coverage, emphasizing their commitment to clarity and support for the provider community.
In this post, let’s dive into three of the top questions, insights, and announcements shared during the session, offering clarity on new health plans, coding, coverage, and other important topics.
1. DMBA’s Provider Portal Enhancements
DMBA has introduced a provider portal with functionalities like pre-authorizations, claim searches, and remittance features. The portal has been live for a year, and additional features will be rolled out over time. Providers can register through DMBA’s website or contact customer service for assistance.
DMBA is retiring its existing four commercial medical plans and introducing four new ones (two PPO and two HSA plans). Providers are advised to review participants’ new ID cards starting next year for updated plan details, including coinsurance and copay structures. The two HSA plans do not have co pays and have certain nuances.
DMBA clarified coverage details for various medical services and billing codes, such as ABA therapy (requires pre-authorization), transitional care management (covered), and select telehealth codes (accepted if recognized by AMA/CPT). Prolonged visit codes, such as 99417, require additional review.
It’s been a busy and rewarding month! We connected with our CHIE customers, sharing valuable insights and updates on the new portal experience. We proudly took part in recognizing the Utah Model of Care as a member of the One Utah Health Collaborative’s Stakeholder Community Board. On top of that, we posted the top five takeaways from our virtual payer panel, attended the Texas Association of Health Plans conference, and shared that Brian Chin will assume the role of Chief Product Officer at Comagine Health, in addition to his position as CEO of UHIN.
The new CHIE portal is live, offering a more modern user interface to access your patients’ longitudinal health records. We’ve created several methods to set you up for success.
CHIE portal users can watch engaging videos that walk you through the new portal features and powerful new tools, and how to log-in through MYUHIN.
Additionally, users can dive deeper into our comprehensive user guide which breaks down every feature step-by-step.
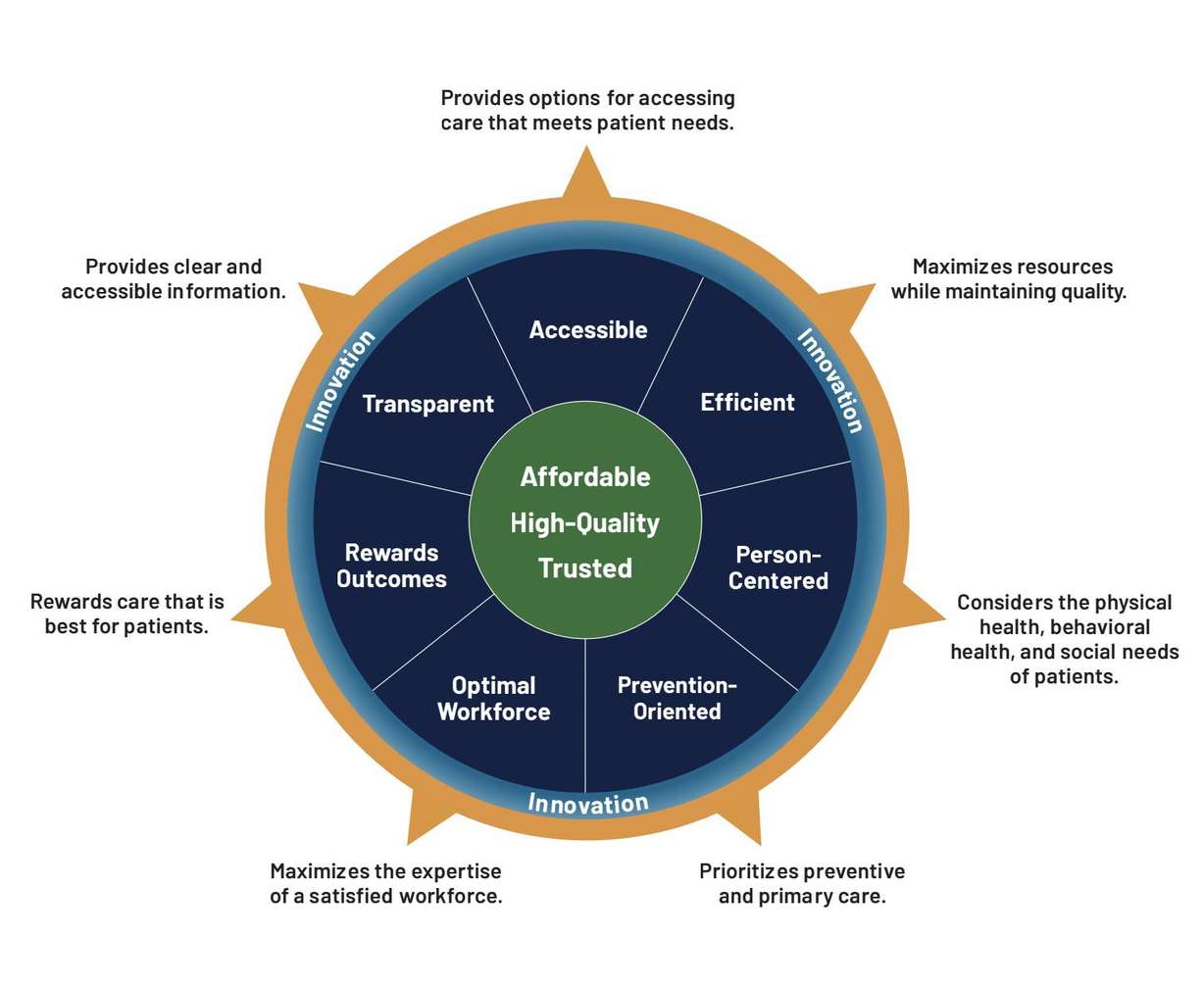
Prioritizing a System that is “Affordable, High-Quality and Built on Trust”
The One Utah Health Collaborative announced the adoption of the Utah Model of Care at the Capitol in late October. The model, developed through statewide collaboration, represents a significant step toward creating a healthcare system that is affordable, high-quality, and trusted for all Utahns. UHIN is proud to be part of the Stakeholder Community Board working with the One Utah Health Collaborative on the Utah Model of Care!
Top Questions and Answers from the Virtual Payer Panel
Dive into five of the top questions and insights shared during the webinar with Lori Weber (Noridian Healthcare Solutions) and Melissa Shoemaker (Select Health), offering clarity on telehealth billing, claims processing, EDI recertification preparation and other essential topics.
We attended the Texas Covered Health Care Conference + Expo Event in Austin, TX from November 4-6.
UHIN will be closed for the Thanksgiving holiday on Thursday, November 28th and Friday, November 29th. We’re thankful for our customers, colleagues, community and partners!
Please note: UHIN Customer Support Holiday Schedule
The UHIN Customer Support call center will be closed on Thursday, November 28th and Friday, November 29th. All regular support issues will be addressed on Monday, December 2nd.
Our on-call team will actively monitor the system to ensure connectivity remains stable. If you have an issue, please contact us through the standard support channels by emailing customersupport@uhin.org. These will be addressed in accordance with our off-hours support policies.
Trainings and Webinars
Watch the CHIE Portal Overview Video
The new platform offers a more modern user interface to access your patients’ longitudinal health records. Learn more about the updated experience in our demo video, including the new dashboard, cards, patient summary, customer support, and future enhancements.
Brian Chin tapped as Comagine Health’s Chief Product Officer
Comagine Health recently announced that Brian Chin will take on the role of their Chief Product Officer, while continuing to serve as CEO of UHIN. In his expanded role, Mr. Chin will lead the development and execution of Comagine Health’s product and technology roadmap, driving their commitment to providing high-quality solutions that meet the changing needs of the clients and the communities they support.
Top Questions and Answers from the Virtual Payer Panel with Lori Weber (Noridian Healthcare Solutions) and Melissa Shoemaker (Select Health)
In the ever-evolving landscape of healthcare billing, staying up-to-date is essential for providers and billing services. In our Virtual Payer Panel, attendees asked questions for two longtime UHIN customers and health plan representatives: Lori Weber, Education Representative for Part B Provider Education at Noridian Healthcare Solutions, and Melissa Shoemaker, Senior Network Engagement Representative at Select Health. Over the course of the webinar, both Lori and Melissa addressed key updates and fielded questions from caregivers of all types.
In this post, let’s dive into five of the top questions and insights shared during the session, offering clarity on telehealth billing, claims processing, EDI recertification preparation and other essential topics.
1. Key Updates on Telehealth Billing
Q: What are the latest updates on POS codes and modifiers for telehealth services? Are there anticipated changes for 2025?
For 2024, providers should use POS 2 for telehealth services provided outside the home and POS 10 for those conducted in the home, eliminating the need for telehealth-specific modifiers. Updates for 2025 will be available after the final rule is released. Providers are encouraged to monitor payer websites for the latest resources, including telehealth pages and webinar archives.
Claims processed with POS 10 will now be reimbursed at the same rate as in-office visits. Adjustments for previously underpaid claims will appear in remittances within 45-60 days.
Q: Can you provide guidance on POS 02, POS 10, and exceptions?
For telehealth services:
POS 10 is used when the patient is at home, while POS 02 applies when the patient is outside their home.
Modifiers are generally not required, but if included, they won’t cause claim denials. However, they may affect reimbursement rates.
Exceptions:
Outpatient therapy services (e.g., physical, occupational, or speech therapy): Use the specific POS 11 (office) as if the patient were seen onsite, and append modifier 95.
Outpatient hospital clinicians: When services are provided to patients at home, use POS 22 (on-campus) or POS 19 (off-campus) with modifier 95.
These guidelines will be detailed in the final documentation.
2. Coverage and Claims Processing for Vaccines and Shots
Q: Is the 90611 JYNNEOS vaccine covered by Medicare Part B?
Yes, Medicare covers the JYNNEOS vaccine for smallpox and MPOX. Billing guidance is available through on-demand webinars that detail the appropriate processes.
Q: What actions are being taken to address flu shot claim denials for certain age groups?
Select Health has identified and is correcting a system error causing flu shot claim denials. Affected claims are being reprocessed automatically. To avoid similar issues, ensure the use of age-appropriate codes and confirm the patient’s Medicare beneficiary status when applicable.
Q: Should 90471 and 90472 still be used for non payable immunizations?
These codes apply to non payable immunizations like tetanus given after an injury. However, for flu and other vaccines, Medicare requires specific G codes for administration. Upcoming webinars will provide further clarification on these requirements.
Q: What steps are involved in the annual EDI recertification process?
Starting in November, providers will be required to verify their trading partner IDs, NPIs, and address consistency across key systems. Email notifications will be sent when recertification is due, ensuring a smooth process for those with up-to-date records.
Q: Is there anywhere online that we can check when the patient had their last preventative visit?
Payers typically allow one preventative billed each year at either 365 days from the previous visit or one in a calendar year.
Lori recommended using the Noridian Medicare portal to track patient preventative visits, ensuring services are billed within covered timelines. Lori emphasized that not all preventative services are annual, with intervals depending on risk levels (e.g., colonoscopies every 5-10 years).
For pediatric visits, Melissa suggested leveraging Select Health’s portal to check service histories beyond the clinic’s records. If more detailed data is needed, she offered to connect attendees with specialized reps for further assistance.
This Virtual Payer Panel highlighted significant updates in healthcare billing, including telehealth billing adjustments, coverage and claims processing for vaccines and shots, the EDI recertification process, and preventative services and eligibility checks. Caregivers are encouraged to leverage available resources from health plans, such as webinars and support services, to stay informed and adapt to these changes effectively.
UHIN will continue to host virtual payer panels with representatives from different health plans throughout the year. Subscribe to the UHIN newsletter and follow us on LinkedIn to stay informed of upcoming virtual payer panels.