“Our life is March weather, savage and serene in one hour” (Ralph Waldo Emerson)
Such was life in the healthcare information technology sector this month. We collectively faced daunting cyber circumstances and peered into an optimistic future filled with the possibilities of A.I., resilient and redundant networks, and healthcare interoperability for all.
Spotlight
Our Response to the Change Cyber Incident
UHIN is dedicated to maintaining interoperability for all payers, providers and partners. When an event as large as the Change Healthcare cyber incident impacts our community, we know we need to serve as a bridge to stable ground. Read more about the actions we’re taking to support our community at this time.
We’re actively supporting Providers by expediting enrollment with Payers to get claims flowing again. Providers can leverage our solutions to create and send professional and institutional claims, submit via SFTP, file tool or online hand-entry, check claims status, manage denials and rejections, and search, view, and download payment information.
We can connect with health plans, so they may receive claims from providers through a direct connection to our clearinghouse. Empower your provider network by elevating your collaboration efforts, securely sharing information and data, and providing better affordable care for your members.
The alarming rise in cyber threats – namely ransomware – highlight the urgent need for enhanced cyber resiliency and robust security measures in healthcare. Read our recent blog post with five ways to reduce your risk and secure personal health information (PHI) from cyberattacks.
HIMSS shared their recap of the 2024 Global Health Conference & Exhibition (March 11-15 in Orlando). Cybersecurity, A.I.,and health equity and access to care delivery were big themes this year. What were you most excited to learn at HIMSS this year?
We’re preparing a series of online trainings for CHIE users this year. Explore our new platform and share feedback with our HIT experts. Stay tuned for updates on upcoming trainings.
Wrapping Up
Thriving in Complexity from the Comagine Health Blog
Comagine Health President and CEO Marc Bennett addresses how the organization has been managing competing tensions while building partnerships to serve as a prime contractor for the 13th Statement of Work in the Midwest CMS QIN-QIO Region 6.
Thanks for spending this extra day going around the sun with us. In February, we dove into the 2023 CAQH Index Report and prepared for the CHIE’s migration to a new platform.
One more thing: For our providers experiencing disruptions in their claims management due to the Change cyberattack, we’re here to help. Please contact us to fast track your enrollment with payers at customersuccess@uhin.org.
Spotlight
Black History Month and American Heart Month
In February we recognized Black History Month and American Heart Month. Here are just a couple ways to support and celebrate these causes throughout the entire year:
For health care professionals and clinicians, use the resources in the Center for Disease Control (CDC) heart toolkit to support their patients, especially women, by listening to their heart.
In Utah? Dive into Utah’s rich black history at the Utah Black History Museum! Find the mobile exhibit across Utah this year or consider donating.
HIT News
The CHIE is Moving to a New Platform!
The new platform empowers CHIE users to better understand patient populations, provide greater care, reduce waste while improving quality, and pinpoint at-risk patients to intervene before their next encounter.
After consulting with our community’s advisory committee, we will be migrating five years of data with the exception of opt out consents, immunizations, allergies, and colonoscopies for which a longer history will be migrated.
Technical implementation is currently underway and we anticipate user migrations will start in Q2 of 2024. We will keep all CHIE users informed of our progress via email.
We published two blog posts sharing our thoughts on the most recent CAQH Index released earlier this month. How did electronic transaction adoption and healthcare administration change in 2023 for both providers and payers? Keep reading to find out.
Our CEO, Brian Chin, recently attended ViVe 2024. Artificial Intelligence was a hot topic this year, as you may have expected. Check out a few photos from the conference here.
Are you going to HIMSS 2024? Let us know what you’re most excited to see while in Orlando next month at communications@uhin.org.
Trainings and Webinars
CHIE platform trainings
We have online trainings coming up for the new CHIE platform. Please sign up for CHIE updates and our Events notifications to add these to your calendar so you don’t miss a thing!
Wrapping Up
Share your story, plus looking ahead to March
Do you have something your peers in healthcare and tech just have to know about? An innovative interoperability solution or point of view? Please email us at communications@uhin.org and we’ll include links to our favorite community content each month.
Next month we’ll attend HIMSS 2024 and help to raise awareness of the risks and symptoms of diabetes on American Diabetes Alert Day (March 26).
Join our monthly newsletter and don’t miss anything!
Question 4: How Does Your EDI Partner Reduce the Burden of Claims Submission for Providers?
Plan members want access to a range of high- quality providers. Without a robust provider network, health plans are challenged to grow membership and differentiate themselves from competitors.
The Council for Affordable Quality Healthcare (CAQH) 2022 Index reported that providers spend ten minutes submitting a single electronic claim on average. For paper, it’s 22 minutes. A large part of this is repetitive data entry. These time blocks add up to significant resource drains in a typical day. Alleviating stressors will reduce payer-provider friction and promote cooperation in your common goal to improve health outcomes for members.
With the right EDI partner, you can streamline operations, reduce administrative burden, and improve your organization’s bottom line. Embracing new technologies and cooperative partnerships can help you gain a competitive advantage and, ultimately, provide better care to members.
Our fourth and final question leads you to ask yourself: “Is my EDI partner providing holistic support to my partner’s and my own organization’s operations?”
Ready to jump to all four questions? Want to see how your EDI partner stacks up? Download our white paper here.
How Does Your EDI Partner Reduce the Burden of Claims Submission for Providers?
Plan members want access to a range of high- quality providers. Without a robust provider network, health plans are challenged to grow membership and differentiate themselves from competitors.
The healthcare industry is becoming more consumer-driven and labor shortages continue to mount. Health plans need to be mindful of provider relationships and the administrative burdens your claims processing may be placing on them.
The Council for Affordable Quality Healthcare (CAQH) 2022 Index reported that providers spend ten minutes submitting a single electronic claim on average. For paper, it’s 22 minutes. A large part of this is repetitive data entry. These time blocks add up to significant resource drains in a typical day. Alleviating stressors will reduce payer-provider friction and promote cooperation in your common goal to improve health outcomes for members.
Your healthcare EDI partner should help you to help providers with an affordable billing tool. Our solution, MYUHIN, reduces repetitive data-entry, and solidifies coding and submissions data to satisfy your processing requirements. Providers can use MYUHIN to submit claims, check patient eligibility, and search, view, and download payment information from any computer, any where.
UHIN is a national EDI network built in 1993 by health plans. We partner with payers and providers across the US. Our approach to EDI and customer service is different. If you’re interest in learning more, please contact us today.
Question 3: Are Providers Frequently Contacting You With Questions About Their Claims?
Health plans constantly seek to optimize their high-performing provider networks which provide value to members and patients. To grow these important networks, payers should nurture their provider relationships through personal attention and cutting edge technology.
This is particularly important at a time of mounting staffing shortages and rhetoric of economic downturns. Additionally, medical claim volume increased by 28% in 2022 as vaccines became available, medical offices reopened and pandemic regulations softened. When you add this up, the need for administrative simplification becomes more obvious for health plans and providers.
Tracking down claims, managing denials and submitting myriad claims can burden staff, compound labor costs and decrease profitability. When your provider network is stressed then your ability to grow as a carrier is impacted. Your EDI partner should automate workflows and manage your trading partner network so your support staff can focus on more strategic priorities, rather than answering phone calls and emails all day long.
Our third question addresses this concern as you ask yourself, “how does my EDI partner stack up?”
Ready to jump to all four questions? Want to see how your EDI partner stacks up? Download our white paper here.
Are Providers Frequently Contacting You With Questions About Their Claims?
When resources are tied up managing claim inquiries, you’re likely underperforming your peers and weakening your organization.
An inability to provide visibility to track and troubleshoot claims in a timely fashion can create financial implications. The increased demand on staff can decrease productivity, which could further delay payments and lead to staff burnout and turnover. Payers must respond to providers within a regulated timeframe, and providers rely on prompt payment for cashflows and their own business growth. Further dissatisfaction amongst providers and members can upend the collaborative nature of interoperability and could drive providers and members away to different plans.
The volume of inquiries to track down claims can burden staff and compound labor costs through the need to hire additional people. The situation can foster negativity between providers and operators, reducing satisfaction for both groups. Your EDI partner should work with you to increase your ability to automate claims processing. Part of this is facilitating a simple, electronic process for providers to submit their transactions and understand the status along the way.
UHIN is a national EDI network built in 1993 by health plans. We partner with payers and providers across the US. Our approach to EDI and customer service is different. If you’re interest in learning more, please contact us today.
Question 2: Can your Clearinghouse validate claims? Can you customize validation to your needs?
Claim validation should be par for the course. Still, many clearinghouses cannot properly validate claims. Much less, health plans are left unable to customize settings that allow for certain transactions while rejecting others. This leads to decreased adoption of auto-adjudication and on-going manual intervention that increases costs and decreases productivity.
SNIP Validation is a common solution for EDI data validation and compliance. There are seven (7) SNIP types and each health plan can tailor type settings to their needs. The right EDI partner works with their health plans to ensure the types are appropriately calibrated and implemented.
This leads to the second question to ask when wondering, “how does my EDI partner stack up?”
Ready to jump to all four questions? Want to see how your EDI partner stacks up? Download our white paper here.
Can your Clearinghouse validate claims? Can you customize validation to your needs?
Ensuring claims are HIPAA compliant and in a valid EDI format before they enter your system is key to streamlining the claims process.
Effective validation reduces administrative workload, mitigates risk of non-compliance, and helps avoid wasted time and provider appeals. SNIP Validation is an important step for pre-adjudication, scalability and profitable growth. Every plan operates at a different level of preparedness. One health plan may be working toward full automation, while another might seek to relieve staff burden to focus on other initiatives. Depending on your systems and goals, an EDI partner can support and modify the validation set-up to support your strategic needs.
SNIP Types
EDI Standard Integrity Testing: Validates the basic syntactical integrity of the EDI submission.
HIPAA Balance Testing: Involves ensuring that amounts reported in different places add up correctly.
HIPAA Inter-Segment Situation Testing: Testing of specific intersegment situations described in the HIPAA implementation guides.
HIPAA External Code Set Testing: Testing for valid implementation guide-specific code set values, as well as other code sets adopted as HIPAA standards.
Product Type/Type of Service Testing: Ensures that the segments (records) of data that differ based on certain healthcare services are properly created and processed into claims data formats.
Trading Partner-Specific Testing: The Implementation Guides contain some HIPAA requirements that are specific to Medicare, Medicaid, and Indian Health.
UHIN is a national EDI network built in 1993 by health plans. We partner with payers and providers across the US. Our approach to EDI and customer service is different. If you’re interest in learning more, please contact us today.
Question 1: Why are you with your current EDI vendor?
Health plans are often led to believe that healthcare electronic data interchange (EDI) vendors and Clearinghouses are utilities. Just a means to an end. It’s true that utilities – such as water – and EDI vendors both follow regulated protocols and move standardized, secure things.
When you turn on the faucet in your kitchen or bathroom, you expect clean, clear water delivered immediately and at your desired temperature. Often it works perfectly. However, you don’t typically choose where the water comes from or the company who provides water to you. You don’t adjust your settings at an infrastructure level and underlying delivery issues may be well beyond your control.
As a health plan, you can select your EDI vendor, enhance your provider network, adjust settings at an infrastructure level, and get ahead of underlying issues. Beneath the surface, health plans can work with expert EDI partners (not just vendors) to navigate turbulent waters together and deliver seemingly fluid experience and impactful outcomes. This process is understandably daunting despite the increased adoption of automated processes.
For this reason, health plans should ask four key questions to understand the value that their EDI vendor is bringing to the table. Our next four blog posts will cover these four simple, yet critical questions for health plans:
With many options out there, why are you with your current EDI vendor? Are they just a vendor in your tech stack or do they serve you as a partner should?
Can your Clearinghouse validate claims? Can you customize validation to your needs?
Is your provider network frequently contacting you with questions? How does this impact your staff, strategy and budget?
How does your EDI partner alleviate the burden of claims submission and simplify your administrative workflow?
Ready to read all four questions now? Want to know how your EDI partner stacks up? Download our white paper here.
Why Are You With Your Current EDI Vendor or Clearinghouse?
Our first post is introspective. We’ll look at the reasons you may be with your current Clearinghouse or EDI vendor, and how they should serve you to meet the strategic objectives of your department and company as a whole. Keep reading about the way it’s always been, and the futurist approach that health plans should take with a key strategic EDI partner.
The Way Clearinghouses Have Worked
Healthcare EDI networks have been built on vendor relationships that can be daunting and confusing, despite best intentions and the increased adoption of automated processes. Vendors offer “sticky” solutions that can entangle health plans with complicated agreements, abrasive onboarding processes, and technology that may not provide meaningful value.
Today, the essence of a partnership can get lost in the complications of healthcare EDI management. We can shift this paradigm by remembering we’re all in this together – from payers to trading partners, and providers to patients.
So, What Keeps You With Your Current Clearinghouse?
Does your partner simplify administrative burden? Do you have visibility into transactions? Do you receive timely, expert guidance on future X12 standards and HIPAA compliant transactions? An EDI partner should be focused on your holistic operations, and not merely transactions (though they should do those well, too). Perhaps it’s time to rethink the status quo.
If your EDI vendor is not serving you as a partner, you may want to consider what this relationship is costing you.
UHIN is a national EDI network built in 1993 by health plans. We partner with payers and providers across the US. Our approach to EDI and customer service is different. If you’re interest in learning more, please contact us today.
Navina Forsythe, MPA, Ph.D., has joined UHIN as our first Chief Data Officer. Dr. Forsythe most recently served as Director of the Center for Health Data and Informatics at the Utah Department of Health. Dr. Forsythe has a Ph.D. in Psychology and a Master’s in Public Administration from the University of Utah. In this new role, she will accelerate UHIN’s efforts to strategically leverage data for client success, and empower interoperability for good across the healthcare spectrum.
As Chief Data Officer, Dr. Forsythe will further UHIN’s mission to support the collaboration of care for patients by providing the right information at the right time in the right format so healthcare professionals may provide the best possible care to patients.
Dr. Forsythe will oversee the development of data and analytics to establish a consistent, coherent approach throughout UHIN, and will tie analytics into all facets of the company. As businesses change and new types of data become available, she will lead efforts to connect the many participants in the healthcare ecosystem to the need for interoperable data and data sharing.
“Navina will help us advance our efforts in leveraging our data management infrastructure by designing curated experiences for the entire organization that map data in ways that inform business choices, and move the power of data into the hands of our healthcare community members. In short, our focus is to give more value through informed insights and actionable information.”
Brian Chin, CEO
Dr. Forsythe is ardently dedicated to data privacy and considers the safeguarding of privacy to be fundamental in all that UHIN does. She is a Certified Information Privacy Manager (CIPM) and served as the Chair of the Institutional Review Board at the Utah Department of Health and Human Services. UHIN is EHNAC accredited and SOC 2 compliant.
Dr. Forsythe has over three decades of experience in health and social services government agencies including clinical work, technology and information systems management, and data management.
As a clinician, Dr. Forsythe has conducted neuropsychological, psychological, cognitive and achievement assessments, provided therapy, group sessions, and cognitive remediation.
As a technology manager, she has overseen development and maintenance of multimillion dollar case management information systems and worked with the Utah Digital Health Services Commission to update and maintain the Utah State Health Information Technology Strategic Plan.
As a Chief Data Officer, Dr. Forsythe has overseen the development of reporting systems and provided information for assessment, policy decision making, process and outcome evaluation, and program improvement.
Every patient deserves a full, dynamic portrait of their care story. We believe in our power to create a more vibrant and complete picture together.
The HIT Conference will feature four tracks with sessions covering topics like population health, interoperability, care delivery, and health equity, as well as popular sessions from previous PES conferences, like “Medicare Hot Topics” with Lori Weber and the Payer Panel. Join other healthcare professionals and attend sessions by esteemed speakers from the State of Utah, Office of the National Coordinator (ONC), University of Utah Health, Amazon Web Services (AWS), Noridian Healthcare Solutions, BYU, AUCH, Comagine, SLCo Health Department, UHIN, and more to be announced!
This event is tailored for professionals across the healthcare ecosystem, such as CEOs, CTOs, CIOs, Chief Medical Officers, VPs, directors, doctors, nurses, administrators, office managers, billers, educators and many more roles at health plans, hospital systems, providers, clinics, higher education institutes, and nonprofit organizations.
PES at HIT
For the first time ever, we’ve combined the annual Provider Education Summit (PES) and the HIT conference into a one-day, hybrid event. PES is an educational event for health plans and providers, billers, office managers, coders, administrators and more. PES will have a dedicated track, Provider Education, at the HIT conference this year.
Welcome Keynote
Rich Saunders
Chief Innovation Officer, Utah
Rich Saunders is Utah’s first chief innovation officer and is charged to help lead the Cox-Henderson administration’s commitment to aggressively upgrade state government efficiencies, innovations, and responsiveness to Utah residents, including a world-class customer experience initiative, and organizing the One Utah Health Collaborative nonprofit. Rich previously served as the executive director of the Utah Department of Health during the COVID-19 pandemic, and before state government, was an entrepreneur for 25 years with extensive experience in multiple verticals and significant sales networks nationwide. Rich has an ongoing passion for leadership, knowledge, organizational health, and service to his community.
Closing Session
Brittany Bowe
Olympic Speed Skater and Medalist
Three-time Olympian, Two-time Olympic medalist, 1,000-meter world record holder
Brittany Bowe led the way for Team USA as the flag bearer for the 2022 Winter Olympic Games in Beijing. She is a Three-time Olympian and Two-time Olympic medalist who gave up her spot in the 500m at the 2022 Winter Olympic Games for Teammate Erin Jackson – recognized as one of the most selfless acts in Olympic history.
1,000-meter world record holder… Reigning 1,000-meter season-long world cup champion… Won seven consecutive 1,000-meter world cup races from December 2018 to December 2019, the longest win streak by a U.S. woman. She helped end a 12-year U.S. women’s drought with an Olympic bronze medal in the team pursuit, and finished top-five in all four of her races at the 2018 Olympics. She is also a Six-time world champion, 20-time world championship medalist and 73-time world cup medalist.
As a gay athlete and LGBTQ+ advocate, uses her platform to promote inclusion and support others. She volunteers as an ambassador for nonprofits Right to Play and Athlete Ally.
Brittany suffered a concussion while training for the 2018 Olympics and was diagnosed with POTS, which means the body does not control blood pressure or heart rate after you stand up. She overcame her fear from that setback and, through an aggressive rehab program, returned to the podium.
Brittany previously played college basketball at Florida Atlantic University and won 32 world championship medals in inline skating before switching to ice. She is dedicated to maintaining a healthy balance between the physical, mental and spiritual aspects of life, and is working toward her yoga teacher certification. Also, Brittany is a cat owner.
Motto: “Practice doesn’t make perfect, perfect practice makes perfect!”
Tracks and Speakers
10:00 a.m. “A Novel Outpatient Complex Care Model – Using Claims Data for Risk Stratification and Evaluation” Dr. Peter Weir | Executive Medical Director of Population Health, University of Utah Health
Read more
A review of the Intensive Outpatient Clinic – highly coordinated and integrated care for Medicaid members with complex mental and medical health problems that result in high utilization.
11:00 a.m. “Partnerships to Increase HPV Vaccine Rates for Utah’s Community Health Centers” Shlisa Hughes | Quality Improvement Director, AUCH
Read more
AUCH is committed to preventing HPV related cancers through improving HPV vaccination rates. AUCH has partnered with Huntsman Center for HOPE, the U of U, Huntsman Cancer Center, the American Cancer Society and the UDHHS, and Utah’s Federally Qualified Health Centers to use automation and interoperability with clinical workflows to improve immunization rates for Utah’s youth. We will share results and innovations from across the state.
Kassy Keen, MPH | Health Equity Bureau Manager, Salt Lake County Health Department
Read more
Health equity has gained increased attention, resources, and support as COVID-19 and social justice movements transform our communities. Often we discuss health equity frameworks, which can be abstract and confusing, offering little guidance around implementation. So, what does it look like to incorporate health equity into systems, programs, and policies in the medical and health field? In this presentation, we will discuss operationalizing health equity, and explore a broad scope of tangible ideas to build capacity, and instill new processes, procedures, and data to create better outcomes for our communities.
2:00 p.m.Orion Health Presentation Chad Peterson | Chief Revenue Officer, Orion Health
3:00 p.m. “Using Analytics to Improve Personal and Population Health“ Sara Hallvik | Vice President of Data Solutions, Comagine Health
Read more
Health data can be a powerful tool in improving both personal and population health, but one must consider several factors first. Data governance determines who and how data is used. Data quality determines whether results can be trusted. Combining data sources increases the complexity but can also increase the power of the data. This opens the way to descriptive, predictive, and prescriptive analytics, where one can harness their data’s true potential.
10:00 a.m. “Why Are We Still Challenged by Identity Matching and Data Quality?Follow Oscar’s Patient Journey” Gregg Church | President, 4medica, Inc.
Read more
Access to accurate, complete, and timely data is one of the most valuable assets in any healthcare organization. The push toward value-based care and population health initiatives including the response to COVID-19 have amplified the need for efficient exchange of quality patient data, filling gaps in information and offering providers and payers a more complete picture of the patient. Quality data improves care coordination, clinical outcomes, and saves lives but can only be achieved with accurate patient identification or matching across multiple sources.
Learning Objectives:
The need for exchanging reliable clinical and administrative data in “real time” for better care coordination and population health management
How patient data is being exchanged securely and reliably for care coordination decisions
How HIE’s and health networks use quality health data to exchange and provide ‘actionable’ data insights in and out of their community
11:00 a.m.“Setting Utah’s Standards: You Hold the Power” Boyd Kreeck | Business Analyst, UHIN
Read more
The UHIN Standards Organization is a nonprofit, broad-based coalition of Utah healthcare insurers, providers, and others, including local government entities. The purpose of the Standards Committee is to develop administrative, technical, and billing standards and specifications based on existing federal and state regulation.
Standards created by the committee and approved by the UHIN Board are provided to the Utah State Department of Insurance, Utah Health and Human Services and published in State Rules and made available to the public at UHIN.org. In addition to developing Utah Standards, the UHIN Standards Committee participates in the development of National standards and guidance.
1:00 p.m. “The Present and Future of HIEs“ Michelle Suitor | Director of the Clinical Health Information Exchange, UHIN
Read more
A discussion on the history of interoperability and an overview of the various standards covered from both the claims and clinical standpoint. This session will explore what that means for Utah, and provide examples of specific use cases.
2 p.m. “Coordinating and Aligning Health IT: An update on nationwide health IT and interoperability goals” Micky Tripathi, Ph.D., M.P.P. | National Coordinator for Health Information Technology, the U.S. Department of Health and Human Services
Read more
Join ONC’s National Coordinator Micky Tripathi for updates on:
ONC’s work to align health IT activities across HHS agencies
How the Trusted Exchange Framework, Common Agreement (TEFCA) will ease information sharing across networks of EHRs and other health IT systems
The continued implementation and enforcement of the information blocking regulations
Data standardization efforts to promote equity, reduce disparities, and support public health data interoperability
And more!
3:00 p.m. “HIE Transformation: It’s About More Than Data“ Mary-Sara Jones | Sr. Business Development Executive, Health & Human Services, Amazon Web Services (AWS)
Read more
The Public Health landscape is changing. It is getting broader and deeper. The global pandemic highlighted fragmentation across and within organizations and the incompleteness of the data available to decision makers. There is a hunger for better, richer, cleaner data to support more holistic decisions and move efforts toward prevention. For many states data modernization and digital transformation will occur in parallel. Immediate updates to shared data infrastructure can provide meaningful insights while updated paradigms of service delivery are reimagined with modern technology to better meet provider and constituent expectations. Health Information Exchanges play a central role in creating and maintaining a connected data ecosystem driving improved patient outcomes and community vitality. This presentation with Natasha Nicolai explores future models for HIEs, how data transformation can provide immediate community impact, and what is required to create the parallel path to digital transformation.
3:00 p.m. “HIE Transformation: It’s About More Than Data“ Natasha Nicolai | AWS WWPS SLG Leader, Health and Human Services Analytics, Amazon Web Services (AWS)
Read more
The Public Health landscape is changing. It is getting broader and deeper. The global pandemic highlighted fragmentation across and within organizations and the incompleteness of the data available to decision makers. There is a hunger for better, richer, cleaner data to support more holistic decisions and move efforts toward prevention. For many states data modernization and digital transformation will occur in parallel. Immediate updates to shared data infrastructure can provide meaningful insights while updated paradigms of service delivery are reimagined with modern technology to better meet provider and constituent expectations. Health Information Exchanges play a central role in creating and maintaining a connected data ecosystem driving improved patient outcomes and community vitality. This presentation with Mary-Sara Jones explores future models for HIEs, how data transformation can provide immediate community impact, and what is required to create the parallel path to digital transformation.
10:00 a.m. “Beating Hypertension, the Silent Killer“ Nickee Andjelic, MS, CHES | Maternal and Infant Health Program Manager, Utah Department of Health and Human Services
Read more
The Utah 6|18 Workgroup is a cross-collaborative workgroup focusing on addressing 6 high-cost and preventable health conditions with 18 evidence-based and cost-effective interventions. For 2022, the workgroup selected to focus on self-monitoring blood pressure (SMBP) by hypertensive patients with clinical support to improve health outcomes and reduce healthcare costs. Hypertension is the silent killer and is a comorbidity and risk factor for a number of other chronic conditions. One in 4 Utah adults have diagnosed hypertension and 15-30% of Utah adults have undiagnosed hypertension. Strong evidence supports that SMBP interventions, when combined with additional support like patient counseling, education, or web-based support, are effective in improving blood pressure outcomes in patients with high blood pressure. Home blood pressure monitors are a covered benefit under Utah Medicaid and many resources are available to support clinic training and member education to encourage accurate SMBP and clinical support.
10:00 a.m. “Beating Hypertension, the Silent Killer“ Dr. Richard Ferguson | Chief Medical Officer, Health Choice Utah
Read more
The Utah 6|18 Workgroup is a cross-collaborative workgroup focusing on addressing 6 high-cost and preventable health conditions with 18 evidence-based and cost-effective interventions. For 2022, the workgroup selected to focus on self-monitoring blood pressure (SMBP) by hypertensive patients with clinical support to improve health outcomes and reduce healthcare costs. Hypertension is the silent killer and is a comorbidity and risk factor for a number of other chronic conditions. One in 4 Utah adults have diagnosed hypertension and 15-30% of Utah adults have undiagnosed hypertension. Strong evidence supports that SMBP interventions, when combined with additional support like patient counseling, education, or web-based support, are effective in improving blood pressure outcomes in patients with high blood pressure. Home blood pressure monitors are a covered benefit under Utah Medicaid and many resources are available to support clinic training and member education to encourage accurate SMBP and clinical support.
10:00 a.m. “Beating Hypertension, the Silent Killer“ Rachel Vasquez | Quality Program Manager, Health Choice Utah
Read more
The Utah 6|18 Workgroup is a cross-collaborative workgroup focusing on addressing 6 high-cost and preventable health conditions with 18 evidence-based and cost-effective interventions. For 2022, the workgroup selected to focus on self-monitoring blood pressure (SMBP) by hypertensive patients with clinical support to improve health outcomes and reduce healthcare costs. Hypertension is the silent killer and is a comorbidity and risk factor for a number of other chronic conditions. One in 4 Utah adults have diagnosed hypertension and 15-30% of Utah adults have undiagnosed hypertension. Strong evidence supports that SMBP interventions, when combined with additional support like patient counseling, education, or web-based support, are effective in improving blood pressure outcomes in patients with high blood pressure. Home blood pressure monitors are a covered benefit under Utah Medicaid and many resources are available to support clinic training and member education to encourage accurate SMBP and clinical support.
11:00 a.m. “The Challenge is HOW not Why: Integrating the Social Determinants of Health in Healthcare“ Dr. Len Novilla | Associate Professor, BYU
1:00 p.m. “Countering Cybersecurity Risks Across Your Organization” Keith Roberts | Information Security Analyst, UHIN
Read more
Presentation on the importance of cybersecurity in healthcare. We’ll look at a recent data breach investigations report, how to stop cybersecurity, and the importance of staff training.
2:00 p.m. “Decentralized Identity and Verifiable Credentials in Health Care“ George McEwan | Chief Strategy Officer (CSO), Department of Government Operations at the State of Utah
Read more
On May 26th, 2011 Google introduced Google Wallet on android phones. Not to be left out of a really good marking term, Apple followed suit on September 19th 2012, launching Apple Wallet. Ten years later and it is still “novel” to pay with a phone. What happened and why does it matter now?
The future of legally binding, decentralized digital identity and verifiable credentials has expanded beyond simple digital wallets and is debuting in government in the near future. This session provides the background you’ll need to participate in the next identity revolution.
3:00 p.m. “Intro and Overview of the One Utah Health Collaborative“ James Wissler | Executive Director, One Utah Health Collaborative
Read more
This intro/overview of the One Utah Health Collaborative will have an emphasis on the barriers and the importance of community alignment regarding interoperability. A panel of innovators, clinicians, and interoperability experts will join Jaime Wissler to discuss the questions of how and why we’re working toward a longitudinal health record.
10:00 a.m. “Motivating for Performance: How Leaders Can Help Teams Find Their Drive” Blake Bishop | Vice President of Data Services, Neovest, a JPMorgan Chase subsidiary
Read more
Intrinsic motivation plays a pivotal role in organizational performance management. Not surprisingly, there is a strong correlation between employee motivation and business success. The factors that drive the desire to perform, however, may come as a surprise to many. In this presentation, we will explore what intrinsic motivation is, why intrinsic motivation matters, and how you as a leader can motivate your team members to perform at their peak.
11:00 a.m. “Medicare Hot Topics” Lori Weber | Provider Relations Specialist, Noridian Healthcare Solutions
Read more
This presentation encompasses updates, important topics and valuable resources to assist your practice with successful Medicare billing.
1:00 p.m.“Life of a Claim: Creation, Rejection, Elation” Joy Cone | Application Support Analyst, UHIN
2:00 p.m.MYUHINClaims Greg Lobato | Group Product Manager, UHIN
3:00 p.m. Payer Panel Representatives from DMBA, EMI, HCU, Noridian Medicare B, PEHP, Regence, SelectHealth, and University of Utah Health Plans
Read more
Q&A session with a panel of provider relations specialists and representatives from national and local, Utah health plans. This popular session answers some of providers most pressing questions. In previous years, questions have included:
Which are the most common errors that keep claims from processing?
What are the procedure codes with modifiers that should be used for phone visits for each insurance company?
Are all the payers reimbursing for Telehealth visits at the same rates as in person visits during the pandemic?
Sponsors
Platinum
Gold
Silver
Venue
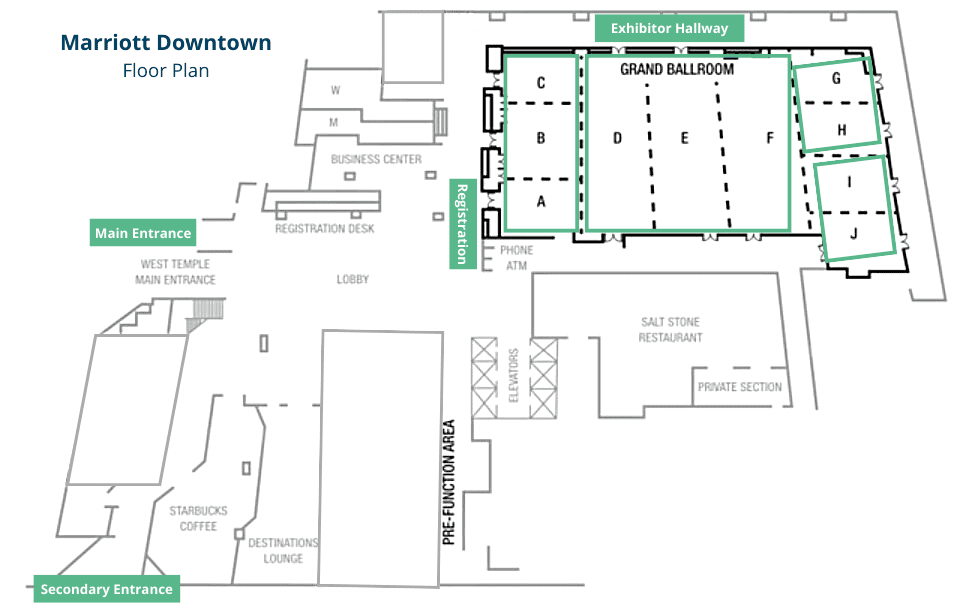
Salt Lake Marriott Downtown at City Creek
75 S W Temple Street Salt Lake City, UT 84101
Free parking for 2022 HIT Conference attendees
REFUND POLICY
We will accept refund requests up to 10 days following the date of the conference. To be eligible for a refund, you must submit via email to events@uhin.org. In your email, include your name, order number, and number of tickets to be refunded, as well as a reason for the refund request.
Once we receive your request, we will review and notify you on the status of your refund. If your request is approved, we will initiate a refund to your credit card or original method of payment.
Please contact events@uhin.org with any additional questions.
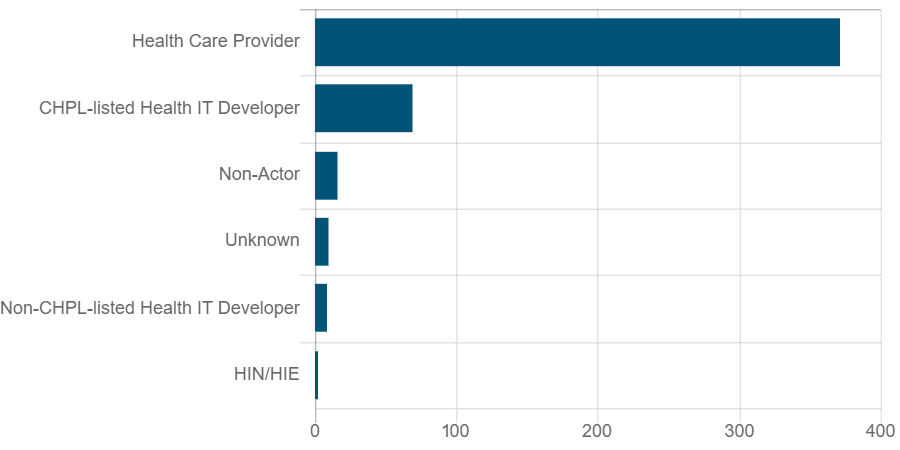
77% of claims submitted identified providers as potential actor; only two claims identified HIEs
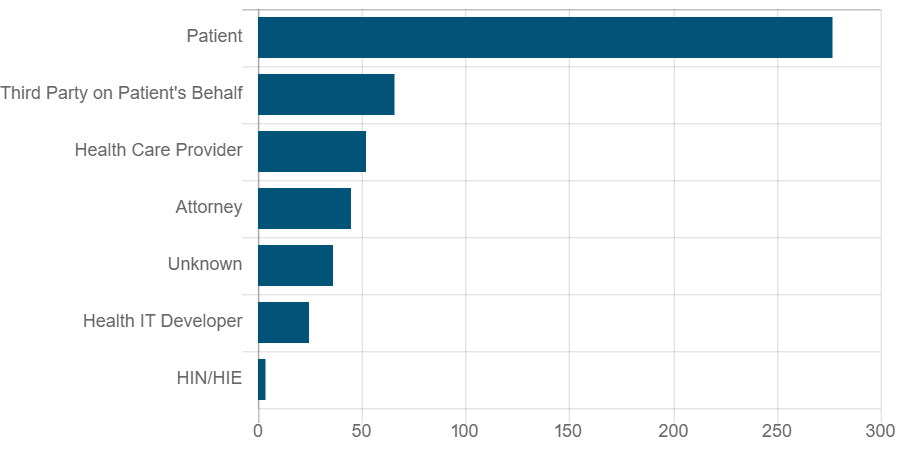
New ONC data shows almost 300 claims of healthcare organizations allegedly blocking access to patient data. Since information blocking regulations went into effect last April, the ONC has received 274 possible claims of information blocking.
Of those claims, 176 were submitted by patients. The majority of claims submitted (211) identified a “health care provider” as the potential actor, with 42 claims naming health information technology developers, and only two claims identifying health information exchanges.
Claim Counts by Types of Claimant
Claim Counts by Potential Actor
Source: Information Blocking Claims: By the Numbers – https://www.healthit.gov/data/quickstats/information-blocking-claims-numbers
“…the circumstances described in the claims may offer insight into potential impediments to EHI access, exchange, or use,” wrote ONC executives Rachel Nelson and Cassie Weaver in a release article. “Though we cannot tell through simple triage whether a particular claim represents information blocking as defined in the regulations, some of the concerns described in the claims we have received appear on their face consistent with examples of practices likely to interfere with access, exchange, or use of EHI that we described in ONC’s Cures Act proposed and final rules.”
In accordance with the 21st Century Cures Act, the ONC seeks to stop certain information blocking practices. New rules were issued in 2020 regarding information blocking regulations with compliance dates going into effect April 5, 2021.
UHIN has long been a proponent of interoperability across the healthcare industry. Our vision is to create a more connected healthcare system that drives innovation, collaboration, and inclusiveness.
The CHIE is an important source of data for Maliheh Free Clinic’s vulnerable patients.
The Maliheh Free Clinic’s patient population is a particularly vulnerable one.
Since Maliheh serves a demographic of patients that sit at up to 200% of the national poverty line, they don’t always have steady access to patient data or even contact information. Their patient population often has limited access to technology, and the clinic itself relies on access to Utah’s two major hospital systems’ EHRs. While this access covers some of their patients, Maliheh staff runs into challenges finding critical information on previous treatment: prescription information, lab results, and other data from other providers and facilities.
With only these tools, Maliheh’s process looks like this:
A new patient with medical data in another system must fill out a Medical Records Request form for each current or past provider. The form is mailed or faxed to each provider, and the patient is evaluated and treated to the best of the clinicians’ ability without previous medical history.
After that, well, the process is a little less clear-cut. Several possible barriers exist at this stage: the form needs to first reach the target provider, and they must actually send back the requested medical information. Sometimes, this requires Maliheh to send the request multiple times to try to get what they need. Once they have the information, staff must then track the patient down so they can provide care- and again, patients may not have steady contact information or addresses, and may have high difficulty in finding time to come back for another appointment. Ideally, Maliheh will provide as much care as possible to the patient on the first visit, but in cases such as these, it’s simply not possible.
Implementing The CHIE to tackle data gaps
In 2018, Maliheh heard about UHIN via an informaticist from one of the Utah health systems. With their small staff (only 12 contracted FTEs), it was going to be difficult to work on integrating a new program into their workflow, but UHIN’s Enrollment Team actively worked with clinic staff to make sure they could get some kind of access to the CHIE, UHIN’s Health Information Exchange tool. The clinic had no extra time to train up any tool experts on their own staff, but UHIN’s team was there for that as well, helping to resolve any usage or technical questions that arose.
Maliheh found that they suddenly had access to patient data and patient matching services for dozens of patients that would have been previously underserved.
As a result of implementing the CHIE as a supplemental data source, Maliheh found that they suddenly had access to patient data and patient matching services for dozens of patients that would have been previously underserved. When a patient’s missing data was in the CHIE, all of the time that their staff spend searching for documentation and trying to send communications could simply be spent providing care to their vulnerable populations. The CHIE was able to help Maliheh avoid long waits for paperwork, lost appointments, and missed care opportunities.
“It’s invaluable to us, it’s like Christmas when we find something in the CHIE. It’s really exciting.”
The CHIE was a solution for the information gaps in Maliheh’s EHR data and their patients’ knowledge of their own care history. With its help, Maliheh is able to provide care to hundreds more patients every year. “It’s invaluable to us,” said Nicole Mohr, Care Coordinator at the Maliheh Free Clinic. “It’s like Christmas when we find something in the CHIE. It’s really exciting.”